Unravelling the Mystery of Panic Attacks: Understanding Causes, Signs, and Coping Strategies
Panic attacks are formidable forces, striking without warning and leaving individuals feeling overwhelmed and powerless. Often misunderstood and stigmatized, these

Advocating for your neurodivergent child in school
Knowing how to best advocate for your child can be overwhelming. Here are some of our top tips to help

Are you visiting 3P for the first time?
We know that experiencing new places and people can be daunting and overwhelming for children so we have created this

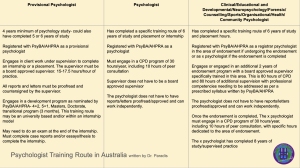
Why are there provisional psychologists working at 3P?
There are a number of provisional psychologists working at Peninsula Paediatric Psychology (3P) and there are a few reasons for

Why is there a psychologist shortage in Australia?
Many have been reflecting on this in recent months. I have been particularly interested in this topic as I opened

Neurodivergent Affirmative Approach: What to expect at 3P?
At Peninsula Paediatric Psychology (3P), we are aiming to offer an assessment experience that is aligned with neurodivergent affirmative professional

What are psycho educational assessments all about?
Parents often come to us as psychologists with a query around ‘we need an assessment’ being slightly unsure about the
Sunday Reflections: Misinformation Risks of Perpetuating the Inequality of Disciplines in Psychology
I am sitting in bed, nicely, quietly, watching the news, contemplating what a day off will bring. Scrolling down on

#Resources 59: A First Aid Kit
I did not anticipate a first aid kit would be such a great hit in the playroom. The kit just

#Resources 58: The Postbox
The playroom is working like a treat so I wanted to share a few resources that I am enjoying working

We did it! Exciting News at 3P!
We have been incredibly busy in the last few months with great projects coming together and a few

Opening a New Venue in Rye!
An awesome news! Opening a new venue in Rye!In January 2022, we will be opening a new venue in Rye,